Ductal (No special type)
Lobular
Tubular/cribriform
Mucinous
Medullary
Papillary
metaplastic
Invasive ductal carcinoma :
is a term used for all carcinomas that cannot be subclassified into one of the specialized types
Carcinomas of "no special type" or "not otherwise specified" are synonyms
produce a desmoplastic response, which replaces normal breast fat (resulting in a mammographic density) and forms a hard, palpable mass
microscopic appearance is quite heterogeneous, ranging from tumors with well-developed tubule formation and low-grade nuclei to tumors consisting of sheets of anaplastic cells
Invasion of lymphovascular spaces or along nerves may be seen.
Advanced cancers may cause dimpling of the skin, retraction of the nipple, or fixation to the chest wall.
About two-thirds express estrogen or progestagen receptors, and about one-third overexpress HER2/NEU
Inflammatory carcinoma :
is defined by the clinical presentation of an enlarged, swollen, erythematous breast, usually without a palpable mass.
The underlying carcinoma is generally poorly differentiated and diffusely invades the breast parenchyma.
The blockage of numerous dermal lymphatic spaces by carcinoma results in the clinical appearance. True inflammation is minimal or absent.
Most of these tumors have distant metastases, and the prognosis is extremely poor
Invasive lobular carcinoma :
consists of cells morphologically identical to the cells of LCIS.
Two-thirds of the cases are associated with adjacent LCIS.
The cells invade individually into stroma and are often aligned in strands or chains.
Occasionally they surround cancerous or normal-appearing acini or ducts, creating a so-called bull's-eye pattern
Lobular carcinomas, more frequently than ductal carcinomas, metastasize to cerebrospinal fluid, serosal surfaces, gastrointestinal tract, ovary and uterus, and bone marrow.
Lobular carcinomas are also more frequently multicentric and bilateral
c/f(clinical factor)
Involvement of the lymphatic pathways may cause localized lymphedema. In these cases the skin becomes thickened around exaggerated hair follicles, a change known as peau d'orange (orange peel).
Outer quadrant and centrally located lesions typically spread first to the axillary nodes.
Those in the inner quadrants often involve the lymph node along the internal mammary arteries. The supraclavicular nodes are sometimes the primary site of spread,
Favored locations are the lungs, skeleton, liver, and adrenals and (less commonly) the brain, spleen
Prognostic factors:
The size of the primary carcinoma. Invasive carcinomas smaller than 1 cm have good prognosis
Lymph node involvement and the number of lymph nodes involved by metastases
The first one or two draining lymph nodes are identified by using a dye or a radioactive tracer, or both. A negative sentinel lymph node is highly predictive of the absence of metastatic carcinoma
Distant metastases
The grade of the carcinoma
The histologic type of carcinoma. All specialized types of breast carcinoma (tubular, medullary, cribriform, adenoid cystic, and mucinous) have a somewhat better prognosis than carcinomas of no special type ("ductal carcinomas").
The presence or absence of estrogen or progesterone receptors. The presence of hormone receptors confers a slightly better prognosis: response (∼80%) to anti-estrogen therapy (oophorectomy or tamoxifen) is seen
The proliferative rate of the cancer. Proliferation can be measured by mitotic counts
Carcinomas with an abnormal DNA content (aneuploidy) have a slightly worse prognosis
Overexpression of HER2/NEU: Overexpression is associated with a poorer prognosis, but also predict response to a monoclonal antibody ("Herceptin") to the gene product.


A. Well-differentiated invasive carcinoma of no special type( NOS). Well-formed tubules and nests of cells with small monomorphic nuclei invade into the stroma with a surrounding desmoplastic response.
B. Poorly differentiated invasive carcinoma of no special type. Ragged sheets of pleomorphic cells without tubule formation infiltrate

Invasive lobular carcinoma. Parallel arrays of small, regular cells with scant cytoplasm infiltrate singly in linear arrays or as small clusters of cells. There is often associated LCIS

The margin of a cancer of the breast revealing tumorous infiltration of the adjacent fatty tissue
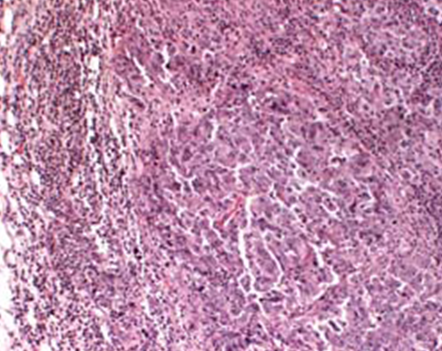
Medullary carcinoma. The cells are highly pleomorphic with frequent mitoses and grow as sheets of cohesive cells. A lymphoplasmacytic infiltrate is prominent

Mucinous (colloid) carcinoma. The tumor cells are present as small clusters within large pools of mucin. The borders are typically well circumscribed, and these cancers often mimic benign masses
0 comments:
Post a Comment