When impulses passes through heart then electrical current also spreads to the surrounding tissues and to surface of body. When electrodes are placed on the surface then it can record the electrical activity . This is known as ECG.

ECG paper
ECG paper: contains small and large squares.
-Each small square is 1 mm and large square is 5mm
-Time is measured along horizontal line and each small square is 0.04 sec and each large square is 0.2 sec.
-Voltage is measured along vertical line and 10 mm is equal to 1 mV
-ECG paper moves at 25 mm/s speed, i.e. 1500 squares/min

ECG leads
3 types of leads:
Horizontal plane leads:
1.Chest leads/precordial leads: V1, V2, V3, V4,V5,V6
Frontal plane leads:
2.Bipolar leads/standard/Einthoven’s leads: I,II,III
3.Augmented unipolar leads: aVR, aVL, aVF
Placement of leads
Augmented leads:
aVR: right arm
aVL: left arm
aVF: left foot
Chest leads
V1: in 4th ICS at right sternal border
V2: in 4th ICS at lft sternal border
V3: midway between V2 and V4
V4: 5th ICS in lft MCL
V5: anterior axillary line in 5th ICS
V6: mid axillary line in 5th ICs
12 leaded ECG/EKG:

Chest leads:

Einthoven’s triangle:



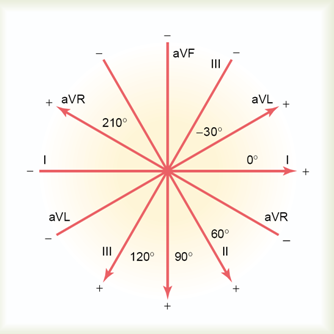
Hexaxial reference system:

The function of the intrinsic conduction system is to initiate and distribute impulses so the heart depolarizes and contracts in an orderly manner from atria to ventricles. * As you must be able to identify the parts of the conduction system and trace the path of depolarization from the SA node to the purkinje fibers, we will review this.
* Since the SA node * has the highest rate of depolarization (75/min) , it starts the process by sending a wave of depolarization * through the myocardium of the atria. When this reaches the AV node * it depolarizes * and causes the Bundle of His * to depolarize.The depolarization travels into the septum through the bundle branches * * and from the bundle branches into the Purkinje fibers * * which cause depolarization of the ventricular myocardium. When the cardiac muscle cells of the myocardium, including the papillary muscles, the ventricles contract forcing blood out of the ventricles. *

Approximately 1% of the cardiac muscle cells are autorhythmic rather than contractile. * These specialized cardiac cells don’t contract but are specialized to initiate and conduct impulses through the heart to coordinate its activity. * These constitute the intrinsic cardiac conduction system. These autorhythmic cells constitute the following components of the intrinsic conduction system:
* the sinoatrial (SA) node, just inferior to the entrance of the superior vena cava into the right atrium,
* the atrioventricular node (AV) node, located just above the tricuspid valve in the lower part of the right atrium,
* the atrioventricular bundle (bundle of HIS), located in the lower part of the interatrial septum and which extends into the interventricular septum where it splits into right and left bundle branches * which continue toward the apex of the heart and the purkinje fibers * which branch off of the bundle branches to complete the pathway into the apex of the heart and turn upward to carry conduction impulses to the papillary muscles and the rest of the myocardium.
Although all of these are autorhythmic, they have different rates of depolarization. * For instance, the SA node * depolarizes at a rate of 75/min. * The AV node depolarizes at a rate of 40 to 60 beats per minute, * while the rest have an intrinsic rate of around 30 depolarizations/ minute. * Because the SA node has the fastest rate, it serves as the pacemaker for the heart. *

An ECG is a recording of the deflection waves caused by depolarization of the heart. * When the SA node * (the pacemaker) * depolarizes * the wave of depolarization that sweeps through the atria is recorded as the P wave * on the ECG. * The P wave indicates depolarization of the atria. * The QRS complex * is caused by depolarization of the ventricles. * Hidden in the QRS complex * is the repolarization of the atria since that occurs while the ventricles are depolarizing. * The T wave * represents repolarization of the ventricles. *

An enlarged QRS * * is indicative of hypertrophy (enlargement) of the ventricles. * * *

A prolonged QT interval * * is indicative of repolarization abnormalities * which increase susceptibility to various ventricular arrhythmias. *

Elevated T wave * is indicative of hyperkalemia, a condition which if not corrected may become life threatening. *

Likewise, a flat T wave * * is indicative of hypokalemia or ischemia. * *

Heart Blocks
Normal ECG

2nd Degree Block:
Not a QRS for each P wave

3rd Degree Block:
No P waves. Rate determined by autorhythmic cells in ventricles



The Frank Starling Law of the Heart states that
'' the more cardiac muscle is stretched within its physiological limits, the more forcibly it will contract. ''
This characteristic of cardiac muscle might be compared to a rubber band. The more you stretch the rubber band, the greater the force that is generated upon release. However if the rubber band is stretched too far, it may break. '' With respect to the heart’s ability to pump blood, increasing volumes of blood in the ventricles increasingly stretch the ventricular myocardium, generating greater force. '' The greater the force, the greater the volume of blood that is pumped out of the ventricle, up to the physiological limits of the myocardium.

ECG waves & genesis
P wave: normally upright , signifies atrial depolarisation
less than 2.5mm height and 0.11 sec duration
QRS complex: ventricular depolarisation N: 0.08 – 0.12 sec
T wave: ventricular repolarisation
U wave: it is positive deflection which comes after T wave. Is due to slow repolarization of interventricular purkinje fiber. Often it is not evident in ECG
R-R interval: distance between two successive R wave
P-R interval : time taken for impulse to travel from SA node to ventricles
0.12-0.22sec
QT interval: total time for ventricular depolarisation and repolarisation
less than 0.42 sec
Axis
Normal axis lies between -30 and +110 degree
Left axis deviation: -30 and -90 degree
Right axis deviation: +110 and +/- 180 degree
Intermediate axis : -90 and +/- 180 degree
Electrical axis of heart


Technique of reading and reporting ECG
1.Heart rate
2.Rhythm
3.Voltage
4.Axis
5.P wave
6.PR interval
7.QRS complex
8.ST segment
9.T wave
10.U wave
11.QT duration
12.Final diagnosis

Determination of axis
Many methods are there
Measure the overal height in leads I and aVF and then plot in graph paper. Then find the vector angle.

Heart rate
HR= 1500/ RR interval in small squares

Uses of ECG
Aids diagnosis, prognosis and treatment
Gives information regarding functioning of atria and ventricles
Identify damage to heart (infarction)
Identify abnormal rhythm and rate
Identify change in size of chambers of heart
Some Abnormalities in ECG
P wave:
a) p wave wide and notched (p-mitral)-left atrial hypertrophy
b) p wave tall and peaked ( p-pulmonale) –right atrial hypertrophy
QRS complex:
Tall QRS- ventricular hypertrophy
Tall peaked T wave- hyperkalemia
Low or inverted T wave- myocardial ischemia
U wave:
Prominent U wave- hypokalemia
ST segment:
Elevated with convexity upward-myocardial infaction
Depressed- angina pectoris
PR interval:
Increased PR interval -Bradycardia
Decreased PR interval- tachycardia
No PR interval- complete heart block

RVH

Coronary infarction

Sinus tachycardia

Ventricular tachycardia following extrasystole

Ventricular fibrillation

ECGs (lead II) showing
abnormal rhythms
A:Respiratory sinus arrhythmia.
B:Sinus arrest with vagal escape.
C:Atrial fibrillation.
D:Premature ventricular complex.
E:Complete atrioventricular block.

Wolf parkinson white ( WPW ) syndrome:
Extra path is formed between atrium and ventricle
Features:
Short PR interval
Wide QRS complex
Delta wave
Heart block:
1.First degree heart block: prolonged PR interval
2.Second degree heart block
a. Mobitz type I b. mobitz type II
3.Complete heart block
0 comments:
Post a Comment