



Global pandemic
HIV 1 and 2: type 2 is predominantly found in west africa
Modes of transmission:
Sexual Transmission
increase in HIV infection in female sex partners of male intravenous drug abusers
The virus is present in semen, both extracellularly and within mononuclear inflammatory cells, and it enters the recipient's body through lacerations or abrasions in mucosa
diseases that cause genital ulcerations, including syphilis, chancroid, and herpes simplex virus.
Gonorrhea and Chlamydia increase the seminal fluid content of inflammatory cells
Female to male transmission has a very low probability compared to the reverse.
Parenteral Transmission
intravenous drug abusers, hemophiliacs receiving factor VIII or IX concentrates, and random recipients of blood transfusion
screening of donated blood and plasma for antibody to HIV, screening for HIV-associated p24 antigen (detectable before the development of antibodies) and heat treatment of clotting factor concentrates have decreased the incidence in this group
nucleic acid testing is a newer technology which might decrease the rate even further
Mother-to-Infant Transmission
inutero, by transplacental spread
intrapartum, during delivery
ingestion of HIV-contaminated breast milk
high maternal viral load and/or the presence of chorioamnionitis
accidental needle-stick injury in health workers: risk of transmission is much lower than hepatitis B
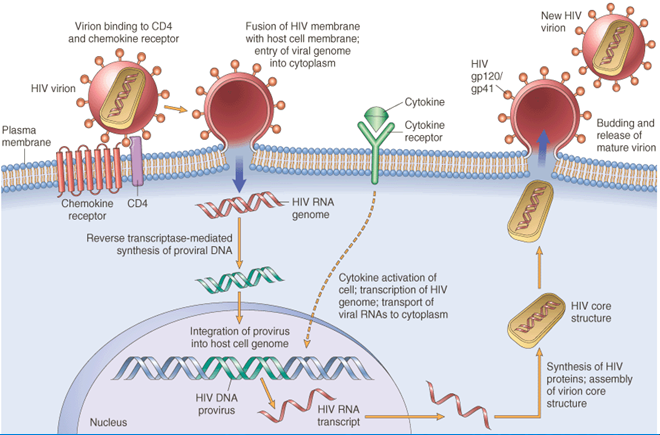
Viral structure:
Virion has major capsid protein(p24), nucleocapsid and lipid bilayer derived from the cell that it infects
viral envelope itself is studded by two viral glycoproteins (gp120 and gp41), critical for HIV infection of cells
2 sets of viral RNA with 3 important genes:
Gag: encodes capsid protein p24, matrix protein p17 and nucleocapsid protein p7 and p9
Pol: encodes polymerase, integrase and reverse transcriptase
Protease is necessary for cleaving all the precursor proteins derived from other genes( Cf protease inhibitor drugs)
Integrase helps in integrating the viral genome into the chromosome of the cell
Env: codes envelope proteins; gp120 mediates CD4 and chemokine receptor binding while gp41 mediates fusion.
Uses host cell transcription and translation mechanism for its protein synthesis
High variability in env gene( envelope glycoprotein which are most important for inducing immune response to the virus) due to low fidelity( high error) of reverse transcriptase
main reason why vaccines cannot be developed
Immunopathology:
CD4 molecule affinity, eg that found in macrophages and dendritic cells: virus binds to the CD4 proteins
Fusion of the viral envelope with the cell mb
Fusion inhibitor- enfuvirtide
Complementary DNA synthesis by reverse transcriptase- the DNA may remain as episome or integrate with the chromosome causing latent infection
Productive infection starts as T cells begin to decline, esp of RES( reticuloendothelial system, including LN,spleen and BM)
Mechanisms of T cell deficiency:
Infected T cells and macrophages form syncitia( giant cells), balloon and die
Cytotoxic CD8 T cells kill infected CD4 T cells
Loss of thymic precursors of T cells
Other viral infections also decrease T cells
Preferential loss of memory T cells cause defective functioning of remaining T cells
CD4:CD8 cell ratio is reversed from 2 to less than 0.5 Other immune cells in HIV:
HIV 1 and 2: type 2 is predominantly found in west africa
Modes of transmission:
Sexual Transmission
increase in HIV infection in female sex partners of male intravenous drug abusers
The virus is present in semen, both extracellularly and within mononuclear inflammatory cells, and it enters the recipient's body through lacerations or abrasions in mucosa
diseases that cause genital ulcerations, including syphilis, chancroid, and herpes simplex virus.
Gonorrhea and Chlamydia increase the seminal fluid content of inflammatory cells
Female to male transmission has a very low probability compared to the reverse.
Parenteral Transmission
intravenous drug abusers, hemophiliacs receiving factor VIII or IX concentrates, and random recipients of blood transfusion
screening of donated blood and plasma for antibody to HIV, screening for HIV-associated p24 antigen (detectable before the development of antibodies) and heat treatment of clotting factor concentrates have decreased the incidence in this group
nucleic acid testing is a newer technology which might decrease the rate even further
Mother-to-Infant Transmission
inutero, by transplacental spread
intrapartum, during delivery
ingestion of HIV-contaminated breast milk
high maternal viral load and/or the presence of chorioamnionitis
accidental needle-stick injury in health workers: risk of transmission is much lower than hepatitis B
Viral structure:
Virion has major capsid protein(p24), nucleocapsid and lipid bilayer derived from the cell that it infects
viral envelope itself is studded by two viral glycoproteins (gp120 and gp41), critical for HIV infection of cells
2 sets of viral RNA with 3 important genes:
Gag: encodes capsid protein p24, matrix protein p17 and nucleocapsid protein p7 and p9
Pol: encodes polymerase, integrase and reverse transcriptase
Protease is necessary for cleaving all the precursor proteins derived from other genes( Cf protease inhibitor drugs)
Integrase helps in integrating the viral genome into the chromosome of the cell
Env: codes envelope proteins; gp120 mediates CD4 and chemokine receptor binding while gp41 mediates fusion.
Uses host cell transcription and translation mechanism for its protein synthesis
High variability in env gene( envelope glycoprotein which are most important for inducing immune response to the virus) due to low fidelity( high error) of reverse transcriptase
main reason why vaccines cannot be developed
Immunopathology:
CD4 molecule affinity, eg that found in macrophages and dendritic cells: virus binds to the CD4 proteins
Fusion of the viral envelope with the cell mb
Fusion inhibitor- enfuvirtide
Complementary DNA synthesis by reverse transcriptase- the DNA may remain as episome or integrate with the chromosome causing latent infection
Productive infection starts as T cells begin to decline, esp of RES( reticuloendothelial system, including LN,spleen and BM)
Mechanisms of T cell deficiency:
Infected T cells and macrophages form syncitia( giant cells), balloon and die
Cytotoxic CD8 T cells kill infected CD4 T cells
Loss of thymic precursors of T cells
Other viral infections also decrease T cells
Preferential loss of memory T cells cause defective functioning of remaining T cells
CD4:CD8 cell ratio is reversed from 2 to less than 0.5 Other immune cells in HIV:
Macrophages with impaired microbicidal activity act as reservoir of HIV virus in different tissues including lungs, brain.
Langerhan dendritic cells of the mucosa bring the virus to the regional LN
Follicular dendritic cells in the LN are also important reservoir
B cells undergo polyclonal activation with hypergammaglobulinemia, but the cells are unable to mount effective antibody response
Defective opsonisation of capsulated bacteria like Meningococcus, Pneumococcus and Hemophilus
Disorders of immune system seen in HIV:
Lymphopenia:
Predominantly due to selective loss of the CD4+ helper-inducer T-cell subset; inversion of CD4:CD8 ratio
Decreased T-Cell Function In Vivo:
Preferential loss of memory T cells Susceptibility to opportunistic infections Susceptibility to neoplasms
Decreased delayed-type hypersensitivity:
Altered T-Cell Function In Vitro:
Decreased proliferative response to mitogens
Polyclonal B-Cell Activation:
Hypergammaglobulinemia and circulating immune complexes Inability to mount de novo antibody response to a new antigen or vaccine
Altered Monocyte or Macrophage Functions:
Decreased chemotaxis and phagocytosis Decreased HLA class II antigen expression Diminished capacity to present antigen to T cells:
Natural history of HIV infection:
Acute phase
Flu like symptoms start 3 to 6 wks after innoculation, representing high level of viremia, seeding of different lymphoid tissue and abrupt fall in CD4 Slowly the immune system of the body tries to clear the infected cells, the CD4 count rises and seroconversion occurs( ie Antibody against the virus is detectable)
Chronic phase
Mildly symptomatic with continued replication of virus and slowly declining CD4 counts, which the body tries to replenish PGL( persistent generalised lymphadenopathy) Minor infections like candida, herpes zoster; aseptic meningitis
Crisis phase
Increased VL( viral load), decreased CD4 Fever less than 1 month, wt loss, chronic diarrhea
After CD4 drops below 500/cmm, AIDS defining diseases including neurological diseases and neoplasms appear
2 types of patients
Rapid progessors
Non progressors
CDC categories:
Mild immunosuppression: CD4 greater than 500
Moderate immunosuppression: CD4 200-500
Opportunistic infections and other AIDS defining illness:
Protozoal and Helminthic Infections
Cryptosporidiosis or isosporidiosis (enteritis)
Pneumocytosis (pneumonia or disseminated infection)
Toxoplasmosis (pneumonia or CNS infection)
Fungal Infections
Candidiasis (esophageal, tracheal, or pulmonary)
Cryptococcosis (CNS infection)
Coccidioidomycosis (disseminated)
Bacterial Infections
Mycobacteriosis
atypical, e.g., M. avium-intracellulare, disseminated or extrapulmonary
M. tuberculosis, pulmonary or extrapulmonary
Nocardiosis (pneumonia, meningitis, disseminated)
Salmonella infections, disseminated
Viral Infections
Cytomegalovirus (pulmonary, intestinal, retinitis, or CNS
infections)
Herpes simplex virus (localized or disseminated)
Varicella-zoster virus (localized or disseminated)
Progressive multifocal leukoencephalopathy
AIDS dementia complex
NEOPLASMS
Kaposi sarcoma
Diffuse large B-cell NHL( EBV associated)
Primary lymphoma of the brain
Morphology of a LN in AIDS:
Normal structure of a LN
Cortex: T cell abundant
Follicles in cortex: B cells, follicular dendritic cells
Sinuses: macrophages
Medulla: plasma cells
In AIDS
Follicular hyperplasia
Later severe involution resulting in atrophic burnt out LN
Invasive cancer of cervix( HPV associated)
Histoplasmosis (disseminated)
Severe immunosuppression: CD4 less than 200
After CD4 drops below 500/cmm, AIDS defining diseases including neurological diseases and neoplasms appear
2 types of patients
Rapid progessors
Non progressors
CDC categories:
Mild immunosuppression: CD4 greater than 500
Moderate immunosuppression: CD4 200-500
Opportunistic infections and other AIDS defining illness:
Protozoal and Helminthic Infections
Cryptosporidiosis or isosporidiosis (enteritis)
Pneumocytosis (pneumonia or disseminated infection)
Toxoplasmosis (pneumonia or CNS infection)
Fungal Infections
Candidiasis (esophageal, tracheal, or pulmonary)
Cryptococcosis (CNS infection)
Coccidioidomycosis (disseminated)
Bacterial Infections
Mycobacteriosis
atypical, e.g., M. avium-intracellulare, disseminated or extrapulmonary
M. tuberculosis, pulmonary or extrapulmonary
Nocardiosis (pneumonia, meningitis, disseminated)
Salmonella infections, disseminated
Viral Infections
Cytomegalovirus (pulmonary, intestinal, retinitis, or CNS
infections)
Herpes simplex virus (localized or disseminated)
Varicella-zoster virus (localized or disseminated)
Progressive multifocal leukoencephalopathy
AIDS dementia complex
NEOPLASMS
Kaposi sarcoma
Diffuse large B-cell NHL( EBV associated)
Primary lymphoma of the brain
Morphology of a LN in AIDS:
Normal structure of a LN
Cortex: T cell abundant
Follicles in cortex: B cells, follicular dendritic cells
Sinuses: macrophages
Medulla: plasma cells
In AIDS
Follicular hyperplasia
Later severe involution resulting in atrophic burnt out LN
Invasive cancer of cervix( HPV associated)
Histoplasmosis (disseminated)
Severe immunosuppression: CD4 less than 200

Natural course of HIV and the different diagnostic modalities
0 comments:
Post a Comment