Protective response of the body to cell injury to remove the noxious stimulus that caused the injury in the first place.
Acute or Chronic if the noxious stimulus persists.
Acute inflammation lasts for minutes to days while chronic inflammation may persist from days to years
Inflammation and repair are the important steps in healing process but the inflammation can cause harm to our native tissues, eg
Anaphylaxis
Autoimmune diseases
Constrictive pericarditis
Cardinal signs of inflammation:
Calor: hot
Rubor: red
Dolor: pain
Tumor: swelling
Function laesa
CellularComponents of inflammation:
Granulocytes:
Polymorphonuclear cells( neutrophils)
Basophils
Eosinophils
Lymphocytes:
B cells and humoral immunity
T cells and cell mediated immunity
Monocytes and macrophages
Endothelium
Fibroblasts
Smooth muscle cells
Mast cells
Natural killer cells


Events in Acute Inflammation:
1.Vascular Events
Vascular dilatation: histamine, bradykinin
Increased vascular permeability and exudation:
Endothelial cell contraction( early) and retraction( late)
Direct endothelial injury: toxins, burn, etc
Leucocyte dependent endothelial injury
Increased transcytosis
Neoangiogenesis: increased gap junctions

2.Cellular events:
Neutrohils initially
Monocytes after 6-24 hours
Rolling and margination
Adhesion: interaction between selectins, integrins and cell adhesion molecules like VCAM
Transmigration by diapedesis
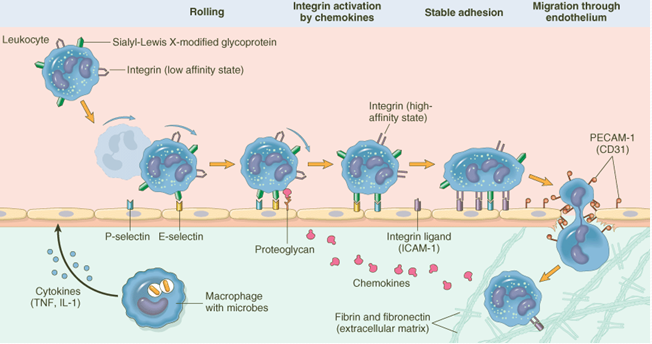
Chemotaxis:
Chemokines: bacterial peptides, C5a, LTB4( Leukotreine), IL 8( interleukin)
Actin myosin interactions in the leucocyte are responsible for diapedesis
Phagocytosis and degranulation
Opsonisation: c3b, IgG, collectins
Oxidative burst
How do neutrophils kill?
Oxidative burst resulting in free radicals
2O2+NADPH ....NADPH.....2O2- ions+NADP+H+
2O2- ions+ 2H+ .....oxidase........ H2O2
H2O2+ Cl-...myeloperoxidase....... HOCl-
Dead organisms digested by lysosomal hydrolases
Bacterial killing also aided by lysozymes and defensins, the latter increase the permeability of bacterial cell.

Body’s defense against free radical injuries
Catalase which neutralises H2O2 into water and O2
Superoxide Dismutase
Glutathione Peroxidase
Antioxidant Vitamins like vitamin A, C and E
Disorders of cellular events of inflammation
Adhesion deficiency
Myeloperoxidase deficiency: Chediak Higasi disease
NADPH Oxidase deficiency: chronic granulomatous diseases
Diabetes
Steroids
leukemia
Chemical mediators of inflammation
Histamine:
Preformed mediator so released early on
Secreted by mast cells and basophils
Secreted in response to
cross linking of IgE during reexposure to allergen in type I hypersensitivity
Anaphylotoxins: C3a, C5a
Substance P: responsible for pain

{kind=link}
Chemical mediators of inflammation
Kinin Cascade:
Coagulation factor XIIa activates Prekallikrein into Kallikrein
Kallikrein activates HMWK( High Molecular Weight Kininogen) into Bradykinin
Coagulation cascade:
Fibrinolytic cascade: tPA activates plasmin
Complement cascade:
Proteases that are nine in number: c1 to c9
Activated by
classic pathway due to Ag-Ab complexes
alternative pathway by microbial LPS or endotoxins
One activated complement activates another
C3a and C5a are anaphylotoxins
C5a is a chemokine
C3b along with IgG work as opsonins
C5b to C9 make the MAC: membrance attack complex


Lysosomal proteases, endonucleases and antiproteases to protect the cells against own enzyme, eg α antitrypsin.
NO( previously called EDRF) by NO synthase
Reactive oxygen species
Arachidonic acid metabolites

Cytokines
Interleukins: more than 20 types
Chemokines
Colony stimulating factors eg GM-CSF
IL 1 and TNFα are responsible for all the acute phase response including fever, cachexia, neutrophil aggregation, septic shock and synthesis of acute phase reactants from liver( eg CRP, ceruloplasmin)



Chronic Inflammation
Outcomes of acute inflammation can either be resolution, chronic inflammation or scarring
Persistence of noxious stimulus causes chronic inflam.
Eg. Chronic viral hepatitis, syphilis, TB and fungi( delayed hypersensitivity), silicosis and other pneumoconioses, autoimmune diseases, etc
Interference in the healing process
3 main components
Mononuclear cell( macrophages) infiltration
Tissue destruction
Repair: by either tissue regeneration or fibrosis
Tissue injury in chronic inflammation is caused by Radical oxygen species, proteases and tissue plasmin activator( tPA)
Fibrosis is a common component in chronic inflammation caused by cytokines like PDGF, FGF, TGFβ, VEGF, etc


Granulomatous inflammation
Type IV hypersensitivity
Attempt at walling off the noxious material
CD4 T helper lymphocyes crucial in recruiting monocytes which turn into macrophages( epitheloid cells) and giant cells
Granuloma with caseous necrosis seen in TB
Other examples are
tuberculoid leprosy
syphilitic gumma
fungal infections like histoplasmosis, blastomyces, cryptococcosis, coccidioides
foreign body like suture materials
pneumoconiosis like silicosis
idiopathic like sarcoidosis
Morphology of a granuloma
lymphocytes( esp CD4 type T helper cells)
macrophages( epitheloid cells, so called because of their resemblance to squamous cells)
epitheloid giant cells formed by the fusion of many epitheloid cells with multiple nucleus in different patterns of arrangement like horseshoe pattern in Langhan’s giant cell seen in TB granuloma.
Necrotic material in centre in case of caseous granuloma as seen in TB
Morphologic types of inflammation
Acute:
Exudative Inflammation: excess fluid. TB lung.
Suppuration/Purulent – Bacterial - neutrophils
Fibrinous – pneumonia – fibrin
Serous – excess clear fluid – Heart, lung
Haemorrhagic – b.v.damage - anthrax.
Chronic inflammation:
with healing.
Granulomatous – clusters of epitheloid* cells eg. TB, Fungus, Foreign body.
Lewis Triple Response:
Flush: capillary dilatation.
Flare: arteriolar dilatation.
Wheal:exudation, edema.

Gastric Ulcer:

Laryngitis:

Mouth Aphthous ulcer:

Acute Enteritis:

Pneumonia:

Neutrophil Margination:

Vascular changes:

Pneumonia - Exudation:

Chronic Inflammation:

Serous Inflammation - Effusion :


Fibrinous Inflammation:

Purulent - Inflammation:



Chronic Inflammation:
Lung Abscess

Granuloma:

0 comments:
Post a Comment