“I had just given birth to my first child and was working in the fields near my village. Suddenly I felt as if my insides were dropping out of me,” the 66-year-old recalled Baffled by what had happened, she told no-one - not even her husband – hoping the problem would go away. But over the years, her prolapsed uterus got worse, to the point that it protruded from her vagina completely, making it difficult for her to walk or even sit upright. She required surgery; a fact prompting this uneducated mother-of-five to finally seek help.
UTERINE PROLAPSE
Definition
- Protrusion of uterus into and out of the vagina from its normal position
- The pelvic structures are divided into 3 compartments : anterior, middle and posterior
- Anterior : urethra /bladder
- Middle : uterus/vault
- Posterior : rectum/anus
Prolapse
- According to the structure underlying it the prolapse is termed as urethrocele
cystocele
uterine prolapse
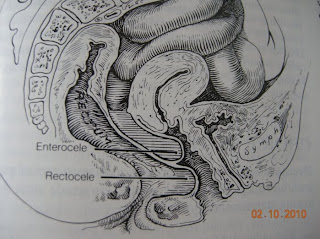
enterocele
rectocele
vault prolpase
Degree of prolapse
- First degree: slight descent of uterus from its normal position but still within the vagina
- Second degree: descent of uterus upto the introitus
- Third degree: protrusion of part of the uterus out of the introitus.
- Procidentia : when the whole of the uterus prolapses out of the introitus.The whole vagina or at least the whole of its anterior wall is inverted



Normal supports
- Axis of the uterus and vagina: anteverted and anteflexed
- Uterus projects into the ant wall of the vagina at an angle so uterus is not in axis with the vagina.
- upper and lower vagina also meet at an angle of 130degree such that the upper half rests on the levator plate

Normal axis of uterus/vagina and the levator plate

Normal anatomy
- Supports of the uterus /vagina
Bony cage
ligaments : Mackenrodts ligament,uterosacral ligament, pubocervical ligament,broad ligament, round ligament
Fascia: endopelvic fascia, Fascia of Denonvillier
Muscles : levator ani and sacrococcygeus (pelvic diaphragm)
urogenital diaphragm
Supports
The muscles of the pelvic floor form the MAIN support of the uterus and vagina .The normal resting tone and voluntary intermittent contraction ,along with contraction of the bulbocavernous muscle constrict the vaginal lumen and elevate the ant. vaginal wall. This is the basis for the Kegel’s exercise.
Levator plate is the median raphe between the anus and the coccyx: the shelf on which the pelvic organs rest. Laxity of this plate leads to prolapse
Muscles of the pelvic floor


Consequences



Aetiology
Congenital : Ehler Danlos Syndrome associated with connective tissue defects; congenital elongation of the cervix
Obstetric : excessive stretching, tearing ,nerve damage that can occur in pregnancy/labour
Menopausal
Iatrogenic : post major surgeries like vaginal and TAH, abdominoperineal resection of rectum etc
Aggravating factors
Chronic constipation, heavy exercise, obesity, chronic cough, weightlifting and pelvic tumours all aggravate the already weak supports
Presentation
- Degree of prolapse bears little relationship to the presenting complaint
- 80% present with complaint of something coming down per vagina
- dragging or bearing down sensation
- backache > on standing, progresses towards the day, relieved on lying down
- difficulty in coitus
- Discharge PV
- tenesmus and constipation sometimes relieved by digital reduction of prolapse – rectocele
- frequency ,incomplete voiding, dysuria, stress incontinence- cystocele
Examination
- vulva examination : laxity of introitus, prolapse type and degree, atrophy changes, ulcer and discharge, rectocele, urethrocele and cystocele
ask patient to cough or strain : stress incontinence
check whether 3rd degree or procidentia,pinch tissue at introitus
PV examination: size of uterus, degree of decent, levator tone, any associated pathology. Diagnose enterocele
Investigation
- No specific investigation for diagnosis
- Most of investigation aaimed at ruling out aggravating factors or complications
eg Urine RE and culture, IVU
chest Xray
swab from discharge
biopsy of non healing ulcer
pap smear
endometrial biopsy in case of bleeding PV
Management
EXPECTANT
PESSARIES
SURGERY
Expectant
- Cases with mild prolapse ,those diagnosed during gynecological examination with minimal or no symptoms
- inform patient of condition
- pelvic exercise
- aggravating factors treatment
- HRT in menopausal women
Pessaries
- Used as early as 2000BC by Egyptians
- Various types have been used over the century
- Main purpose is to stretch the vault and hold the uterus up. Some amount of inherent tone is needed for the ring to remain in place
- Ring Pessary commonly used : rubber
- changed every 3 monthly
- temporary method of treatment
Types of pessaries

pessary
- If patient refuses surgery
- Patient medically unfit for surgery
- Temporary measure while patient waits for surgery
- Ulcer : helps in healing of the ulcer
- in pregnancy : early pregnancy
- in puerperium
Its use is not without problems
Surgery
- Type of surgery depends on the reproductive goal, age of patient , surgical fitness, type of prolapse and severity, need for preservation of coital function, assocaited other pelvic disease
- symptomatic cases especially those with mod to severe degree of prolpase
uterus preserving
anterior colporrhapy
post colpoperineorraphy
Manchester Operation
Colpocleisis
Le Forts Operation
Sling operations
Fothergill or Manchester operation
- Dilation and curretage
- anterior plication of the cardinal ligaments
- amputation of cervix and reconstruction
- ant colporraphy
- PFR
ideal in women with congenitaly elongated cervix
Lefort operation:
rectangular folds of vaginal wall from ant and post wall are removed and the raw surfaces are sutured together
can even be done under LA ,suitable in old medicaly unfit lady with prolapse
Colpocleisis : concentric sutures placed in vagina which is used to close the vagina and so hold up the prolapse
Sling operations
- for young women with severe prolapse who want to conserve the uterus
- objective of operation is to buttress the weakened supports of the uterus with substitutes like fascial or synthetic material.
eg : sacrohysteropexy: post junction of uterus and cervix is attached by mesh to the ant longitudinal ligament of sacral vertebrae
abdominocervicopexy: musculofascial strips from ant abd wall inserted onto isthmus of uterus
Operations
- Uterus is removed
- Vaginal Hysterectomy with Ant Colporraphy with pelvic floor repair
0 comments:
Post a Comment