Various systems affected
- Reproductive organ changes
- Cardiovascular changes
- Hematological changes
- Respiratory changes
- Changes in urinary system
- Endocrine organ changes
Reproductive organs
- Vagina
- Cervix
- Uterine corpus
- Breast
Vagina
- Increased vascularity and hyperaemia of mucosa
- Increased thickness of mucosa, increased loosening of connective tissue, hypertrophy of muscles -increase in length and distensibility
- Increased vaginal secretions, acidic medium with increased lactobacillus
Cervix
Pronounced softening and cyanosis –after a month of pregnancy (Goodell’s sign)
- increased vascularity & edema
- cervical glandular hypertrophy /hyperplasia
- rearangement of collagen with decrease in mechanical strength at term
Thick mucus – bloody show at labour
Uterus
Hypertophy and dilatation
normal 70gm ----------------10ml cavity
pregnant 1100gm -------------5litres
Increase in size is contributed by
muscle hypertrophy, hyperplasia, stretching
increased vasculature/lymphatics
Firm uterus –> soft in early pregnancy -> distensible muscular sac in late pregnancy
- Change in size & shape
pear shaped –> almost spherical at around 3rd month-> oval in shape in later pregnancy
Size : hens egg at 6 weeks
cricket ball at 8 weeks
Asain pear at 10 weeks
out of pelvis after 12 weeks
- Dextrorotation ? Due to rectosigmoid on the left side
Change in contractility
painless contractions from as early as first trimester
detectable by second trimester ( Braxton Hicks)
painful, regular, increasing in intensity and frequency – labour
- Uteroplacental flow
uteroplacental flow is increased in pregnancy
450-750ml/min late in pregnancy. This is required to maintain an adequate placental perfusion.
- Endometrium
Decidual reaction –3 layers differentiation
trophoblast formation
Isthmus
- Hypertrophy ,elongation in first trimesterto three times its length
in second tri- gradually taken up and incorporated into the uterine corpus.
The circular muscles in region act as sphincter
Respiratory changes
ANATOMICAL
* diaphragm rises by 4 cm
* compensatory increase in thoracic transverse diameter by 2 cm
* Increase in circumference of the thorax
Pulmonary function
- Respiratory rate – relatively no change
- Vital capacity (3.2L) – almost unaltered
- Pulmonary vascular resistance is decreased (Progesterone effect)
- Residual volume – decreases by 20%
- Tidal volume (485ml) _ increases by 40%
- Airway conductance is increased, oxygen requirement is increased
Respiratory
Increased respiratory effort (dyspnoea)
arterial PCO2 is decreased and O2 is increased
facilitates O2 transfer to fetus
Respiratory diseases may worsen in pregnancy as O2 requirement in pregnancy increases
Urinary system
Kidney:
increase in size by 1 cm
dilatation of pelvis, calyces and ureter
GFR (50% increase) increases throughout pregnancy
renal perfusion increases by 25-50% in early pregnancy
So serum urea and creatinine values decrease in normal pregnancy.
Urine
- Glycosuria- decrease in renal threshold,
persistent glycosuria – possibility of DM
- Proteinuria - not evident in pregnancy
except in slight amounts after labour/puerperium
- Hematuria – UTI, difficult labour, instrumental delivery
Ureter
Hydronephrosis and hydroureter due to effect of progesterone
RIGHT SIDE more than left
* cushioning by the sigmoid colon on the left
* right ovarian vein crosses the ureter obliquely
Elongation , angulation and lateral displacement of ureters by gravid uterus
Comes back to normal in 6 – 8 weeks post partum
Bladder
Few changes before the 4th month
Gravid uterus, pelvic congestion - causes
bladder trigone to be elevated, thickening of interureteric ridge and also rest of bladder,
increased tortuosity and size of vessels in mucosa
In late pregnancy, especially engaged head pushes base of bladder forward increasing the congestion , oedema and increase susceptibility to trauma and infection.
Post delivery esp vaginal – stress incontinence by urethral sphincter damage
CARDIOVASCULAR
ANATOMICAL
Heart is elevated and rotated towards left- causes apex to move more lateral and cardiac silhouette to appear larger
HEART SOUNDS
Splitting of first sound
Third sound heard loudly
Systolic murmur in 90% cases - disappear shortly after delivery
Continuous murmur (10%) – b/o increase in breast vasculature
ECG –left axis deviation
Cardiac output
Increase due to increase maternal weight, blood vol. increase, increased BMR
CO = SV X HR (minimal change)
Starts from early pregnancy (10weeks), increases cont upto 28weeks –
Max at 32 weeks – slight decrease towards term - increase in labour – decreases in postpartum
CO 4.5L - 6.2 L in pregnancy(30-40%)
CV changes
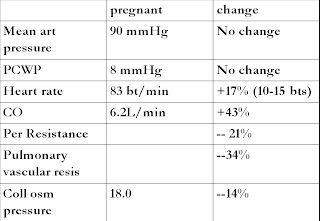
Blood pressure – remains same due to decrease in peripheral resistance
Mid pregnancy drop of 5-10 mmHg can occur due to pooling of blood in uteroplacental circulation.
More marked in hypertensives
Towards term –supine hypotension – gravid uterus compresses IVC – decreases venous return -hypotension
Venous system – pressure by gravid uterus and progesterone
- distensibility of veins
|
pedal oedema,varicose,haemorrhoids
thrombosis
Circulation – increased blood flow to uterus, kidneys, skin & lungs
In uterus 50ml /min in non pregnant to 750ml/min at term
Haematological changes
Blood volume : increases by 40%
* meet demand of increased uterus
* protect mother and fetus against deleterious effects of decreased VR
* safeguards the mother against effects of blood loss in delivery
Blood volume - increased plasma volume (40%)
- increased RBC volume (33%)
Haemodilution-
mean Hg falls from 13.3gm/dl in non preg to 10.9g/dl in pregnant .

<11gm/dl of Hg – anaemic
Hypercoagulable state
increase in plasma fibrinogen ,with increased rouleaux formation, decreased fibrinoltic activity

Haematological
- WBC increased - 5 to 12000/cmm in pregnancy
14-16000/cmm in puerperium
even up to 20000/cmm
- ESR increases (x4 times)
- Blood protein : serum albumin level decreases by 30 % . Plasma protein conc decreases –decreased colloidal oncotic pressure
Iron metabolism
Iron content is decreased – increased erythropoiesis & increased transfer to fetus
Total iron needed
Increase in RBC (450ml) = 500mg
transfer to fetus = 300mg
insensible loss = 200mg
Total = 1000mg
Compensatory efforts are not sufficient
Metabolic changes
- Weight gain : total about 12.5kg
- 1 lb/week after 20 weeks

Water metabolism
- Fundamental change in pregnancy is fluid retention.
- Total about 6.5L of fluid is retained

Protein metabolism
- Protein gain in pregnancy
500gm –fetus /placenta
500gm – contractile proteins, breast, Hb and plasma proteins
Protein supplementation in diet is needed, but along with carbohydrate & fat
Carbohydrate metabolism
- Potentially diabetogenic
mild fasting hypoglycemia
post prandial hyperglycemia
hyperinsulinemia
All this to ensure a maintained supply of glucose to fetus
Insulin resistance could be due to ? Insulinase enzyme
Endocrine changes
- Pituitary
increase in size
increase in GH – weight gain in preg
increased ADH and oxytocin
leading to oedema of pregnancy
Thyroid gland
- Increase in size –hyperplasia of gland
- TSH increase which causes hyperplasia, increase in BMR beginning from the third month
- Increased Estrogen- increased TBG conc and binding capacity- increased serum protein bound iodine and Increase in circulatory T 4 and T 3
Adrenal gland
- Slight increase in size-mainly cortex
- Increase in level of serum cortisol, aldosterone
- which could be responsible for the edema of pregnancy
Important Questions:
Q1.During CS, anaesthetist puts the patient in the left lat position. Why?
Answer: Supine Hypotension
Q2.In a heart dis prgnant patient –most dangerous time is ?
Answer: Second stage of labor
Q3.USG done in a pregnant woman at 30 weeks shows hydronephrosis ? What will you do?
0 comments:
Post a Comment