
Structure of kidney 6-8 calyx, 12-15 renal pyramids in medulla, cortex extension between medullary pyramid are called renal columns.
Cortex+Medulla=Parenchyma
Line joining base of Pyramid differntiates the cortex from medulla
Scan Planes
Flank scan
Upper abdominal transverse scan
Lateral upper abdominal longitudinal scan
Scanning Technique
Fasting not required, well hydration required, long. & transverse scan of kidney.
Sonographic anatomy and normal findings:
The kidneys are located in the retroperitoneum on the iliopsoas muscles. Their longitudinal axes point laterally downward. Their lower poles are directed forward and lateral.
An imaginary line joining the bases of the medullary pyramids separates the cortical substance of the kidney from the medulla.
CEC appears Hyperechoic and consists of vessels, connective tissue, renal sinus fat, and the actual renal pelvis.
Normal values:
Length100–115 mm, width 50–70 mm, Thickness 30–50 mm.
Parenchyma: The parenchymal–pelvic ratio (ratio of the combined anterior and posterior parenchymal thickness to the CEC) is 1.7 up to 60 years of age and 1.1 after age 60.


Normal right kidney – L = Liver, MP = hypoechoic medullary pyramids, C = Renal Columns
Scanning protocol
Transducer: 3.5–5.0 MHz
Patient generally supine. Left lateral decubitus occasionally used (esp. left kidney)
Right kidney: The lower pole is occasionally obscured by the right colic flexure but is accessible to scanning from the posterior side.
Left kidney: Scanning from the posterolateral side is advantageous as it avoids overlying gas in the colon and gastric fornix.
Always scan the kidneys during inspiration and expiration to ensure that they are completely visualized (rib shadows and bowel gas are often troublesome) and move normally with respiration (i.e., are not fixed by perirenal abscesses).
Both kidneys are systematically surveyed in longitudinal and transverse planes.
Causes of large or small kidneys
Small kidneys:
May be constitutional or may result from hypoplasia or ectopia, making the organs difficult to locate
Large kidneys:
May be constitutional or may result from duplex kidneys, unilateral aplasia, acromegaly, or compensatory enlargement of the remaining kidney after nephrectomy

Causes of difficult visualization or nonvisualization
Ectopic kidney:
Located along the path of its normal ascent, usually in the lesser pelvis near the iliac vessels; “lower abdominal mass”
Unilateral renal agenesis:
Characterized by enlargement of the contra lateral kidney
Hypoplastic kidney:
Careful inspection of the renal fossa in a close-up view should reveal a small kidney with normal-appearing parenchyma.
Atrophic kidney:
Shrunken kidney that displays abnormalities in its contours, internal echo pattern, or both
Renal fusion anomaly:
A bilateral “horseshoe kidney” initially appears as two normal kidneys, but the lower poles are found to be fused across the midline in the lesser pelvis.

partial horseshoe kidney on the left side (K). AO = aorta, V = compressed vena cava, M = lumbar muscle, L = liver
Acute Pyelonephritis:
Eighty percent of infections are caused by Escherichia coli.
The remainder of cases is mostly caused by other gram-negative organisms, including Klebsiella, Proteus, Enterobacter, Pseudomonas, Serratia, and Citrobacter.
Fungal infections are also present especially in the setting of diabetes, immunosuppression
Present with localized complaints of flank pain and costovertebral angle tenderness accompanied by generalized symptoms of fever, chills, nausea, and vomiting.
In addition, these findings may be accompanied by further lower urinary tract symptoms, including dysuria, increased urinary frequency, and voiding urgency
Laboratory abnormalities indicative of the underlying infection can be expected, including neutrophilic leukocytosis on the complete blood count and elevated erythrocyte sedimentation rate
In severe infection elevated S. Creatinine may be present due to interference with Renal functions.
Urine cultures, which should be collected before starting antibiotic therapy, will almost exclusively demonstrate infection from gram-negative bacteria.
Chronic Pyelonephritis:
A common clinical presentation is anemia, leukocytosis, and flank pain.
A majority of patients have urinary obstruction due to nephrolithiasis, at times even a staghorn calculus.
US reveal calculi, hydronephrosis, or a renal tumor.
Ultrasonographic features of Acute pyelonephritis


Pyelonephritis. Transverse gray-scale (A) and color flow Doppler (B) sonography of the right kidney demonstrate two wedge-shaped areas of decreased echogenicity (arrows) in the renal cortex with absence of color flow, consistent with multifocal pyelonephritis
Renal tuberculosis
80% cases are respiratory TB, 20% may be extra pulmonary.
Latent foci may result in kidney lesions many years following primary infection, though only 5% of patients who have active tuberculosis will have cavitary lesions in the urinary tract
Often patients will present asymptomatically, even in cases of advanced disease. If disease involves the bladder, symptoms of urinary frequency may result. One quarter of patients will present with findings of a unilateral poorly functioning kidney.
Diagnosis of urinary tract tuberculosis can be established through a urine culture that demonstrates growth of M tuberculosis
These patients have a sterile pyuria, microscopic hematuria, and an acidic urine
Ultrasound findings in the diagnosis of renal tuberculosis have traditionally been described as limited
Granulomatous mass lesions in the renal parenchyma can be seen as masses of mixed echogenicity, with or without necrotic areas of caseation and calcifications
In addition, findings of mucosal thickening of the renal pelvis and ureter, ureteral stricture, and hydronephrosis are seen

Longitudinal gray-scale ultrasound of the right kidney demonstrates hypoechoic areas (arrows) in the renal cortex suggestive of lobar caseation in this known case of tuberculosis

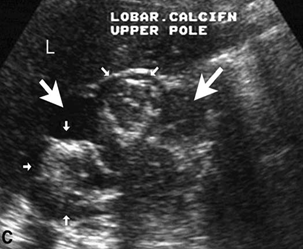
Longitudinal gray-scale sonography of the kidney in another patient who has renal tuberculosis demonstrates hypoechoic areas of caseous necrosis (large arrows) with dense peripheral calcification (small arrows).
Renal adenoma
Benign counterpart of RCC
renal cortical glandular tumors of smaller than 3 cm rarely metastasize
Most pathologists consider these small renal cortical tumors to be premalignant or potentially malignant and believe that tumor size is not a valid differentiating criterion

Renal adenoma. a Intensely hypoechoic mass with smooth margins.
Renal cell carcinoma
RCC is the most common primary malignancy of the kidney. It accounts for 2% of all malignancies.

Imaging cannot differentiate the different histologic types of RCC.
The incidence of RCC increases in acquired cystic disease of the kidney
classic clinical triad of hematuria, abdominal pain, and abdominal mass is seen in less than 10% of patients.
About 20% to 40% present with paraneoplastic syndrome, which includes anemia, fever, hypertension, hypercalcemia, and hepatic dysfunction
Most common sites of metastasis include Lungs and Bones.
Role of USG:
The goal of imaging is detection, diagnosis, and staging of RCC
Ultrasonography is less sensitive in detecting small renal lesions, especially those that do not deform the contour of the kidney. The sensitivity of CT and USG for detection of lesions 3 cm and less is 94% and 79%, respectively
Renal cell carcinomas range from hypoechoic to hyperechoic compared to normal renal parenchyma
Ultrasonography is also less accurate than CT and MRI in staging of RCC
ultrasonography is still the initial imaging modality for screening and characterization of renal mass lesions
The sonographic spectrum of RCCs varies from hypoechoic to hyperechoic solid mass lesions
RCCs 3 cm and smaller are predominantly hyperechoic.
 Longitudinal gray-scale sonography of the right kidney demonstrates an iso- to hypoechoic mass arising from the lower pole
Longitudinal gray-scale sonography of the right kidney demonstrates an iso- to hypoechoic mass arising from the lower poleRenal Stones
Urolithiasis, the presence of renal calculi within the urinary tract, is the most common cause of extrarenal obstructive uropathy
Hydronephrosis refers to the structural change, describing a dilatation of the calyces and renal pelvis. Hydroureter, or ureteral dilatation, sometimes accompanies hydronephrosis
Chemical Composition
Calcium-containing, or calcareous, stones are the most common type, accounting for 60% to 80% of all uroliths, followed by uric acid stones, which account for 5% to 10%
Calcareous stones are typically uniform in density and are easily detected on plain films and noncontrast CT.
USG picture
Ultrasound may detect with relative confidence stones greater than or equal to 5 mm
Calcareous stones which are more common are very echogenic on ultrasound and we may find them in the renal pelvis or in the renal calyces.

Right renal nephrocalcinosis. Longitudinal
US scan identifies numerous discrete hyperechoic foci in the kidney
Glomerulonephritis
Glomerulonephritis is an inflammatory condition which affects the glomeruli of the kidney.
It may be either acute or chronic, and frequently follows prolonged infection.
Patients may present in acute renal failure, with oliguria or anuria, or with features of nephrotic syndrome such as oedema, proteinuria and hypoalbuminaemia
Ultrasonography Changes:
In the acute stages the kidneys may be slightly enlarged; changes in the echogenicity of the cortex may be observed.
In the chronic stages the kidneys shrink, become hyperechoic, lose cortical thickness and have increased corticomedullary differentiation
Renal tb
By hematogenous route
May produce irregular thickening of bladder
Loss of corticomedullary junction
In 25% cases,calcification is seen
Renal artery thrombosis
Develops an acute flank pain ,haematuria
Absebt arterial flow using colour doppler
Wedge shaped hypoechoeic focal masses
ACUTE GLOMERULONEPHRITIS
Increased cortical echogenicity with medullary sparing.
Hydronephrosis
Separation of renal sinus echo by dilated calyces
Sometimes with full bladder or pregnancy,may have pseudohydronephrosis
In severe hydronephrosis,cortical thinning occurs.
RENAL CALCULI
Stone as small as 1.5 cm can be seen
Calculus of size >6cm will cast shadow
TRANSPLANT KIDNEY
Commonly seen at the iliac fossa
URETER
25 cm length,extraperitoneal,sonographically normal ureter isnot seen
Vesicoureteric stone very common in clinal practise.
0 comments:
Post a Comment